
Copyright 2007
By Gregory R. Waryasz, MD
The clavicle of the musculoskeletal system is characterized by being the bone that connects the upper limb to the trunk. It is also known as the collar bone.
It is part of the upper limb. The clavicle is part of the acromioclavicular and sternoclavicular joints. It consists of bone and cartilage tissue once mature.
Its unique structural features include its being a double curve when viewed in the horizontal plane. It is S-shaped with the medial end being convex forward and the lateral end being concave forward. The lateral portion of the bone is thinner than the medial end. Although classified as a long bone by anatomists, it has no medullary canal.
The surface texture of the clavicle changes depending on the location. Superiorly the clavicle is smooth as it lies deep to the platysma. Inferiorly the clavicle is rough to allow for ligaments to attach to it.
The conoid tubercle is the site of attachment of the conoid ligament. The trapezoid line is where the trapezoid ligament attaches. The subclavius muscle attaches at the subclavian groove which is located in the medial third of the clavicle shaft. Most medial is the impression for the costoclavicular ligament where the attachments for the ligaments to the sternum’s manubrium are located.
Ligaments that attach to the clavicle are located distally and proximally. Distal ligaments include the acromioclavicular ligament that connects the scapula’s acromion to the clavicle and the coracoclavicular ligaments that connect the coracoid process of the scapula to the clavicle. The coracoclavicular ligaments are the trapezoid and the conoid. The proximal ligaments are the anterior and posterior sternoclavicular ligaments, intraclavicular ligament, and the costoclavicular ligament.
The blood supply to the clavicle is periosteal, there is no nutrient vessel.
The clavicle is the first bone to ossify at the 5th week of gestation. The ossifaction center at the sternal end fuses between 22 and 25 years of age. The clavicle as well as all other bones, muscles, and ligaments of the body are derived of mesodermal origin in embryo.
The function of the clavicle is to be a strut that connects the shoulder and the trunk. This allows the shoulder to have optimal function as it allows the arm to be away from the trunk. The medial portion of the clavicle helps to protect the brachial plexus, subclavian and axillary vessels, and the superior aspect of the lung. The clavicle also helps with transmitting shocks from the upper limb to the axial skeleton.
Common diseases of the clavicle include arthritis, fracture, separation/dislocation, tumor, osteomyelitis, and congenital absence.
Arthritis can occur at either the acromioclavicular or sternoclavicular joint. Common arthritis types that can occur at these locations include osteoarthritis and rheumatoid arthritis.
Fracture of the clavicle is common to occur in a wide variety of individuals. Infants can suffer birth trauma resulting in a clavicle fracture.
Dislocation or separation of the acromioclavicular or sternoclavicular articulations can occur with trauma.
Osteomyelitis is an infection of the bone usually due to bacteria.
Tumors can either be primary or from metastasis. A few primary tumors that can occur in bone include leukemia, lymphoma, neuroblastoma, osteoblastoma, osteosarcoma, osteoid osteoma, enchondroma, and Ewing’s Sarcoma.
Congenital absence of the clavicle can occur. It may not significantly affect shoulder function.
Commonly used diagnostic procedures include clinical history, physical exam, x-ray, MRI, bone scan, and CT scan.
It is usually treated with internal or external surgical fixation or non-operative approaches for fractures. Dislocations and separations are usually treated non-operatively with a sling, however can require surgery in some instances. Tumors can be treated with surgery, chemotherapy, and radiation. Arthritis is treated initially with physical therapy, NSAIDs, and steroid injections. Osteomyelitis is treated both surgically and with antibiotics. Congenital absence may or may not require treatment.
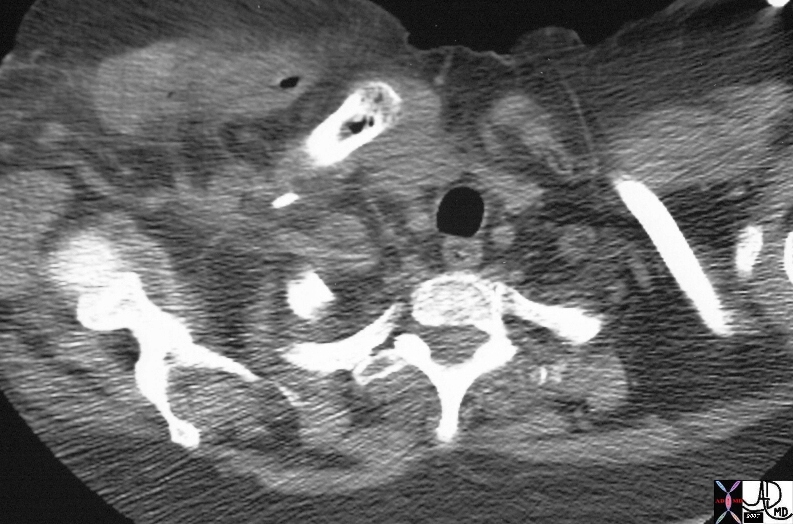
Pectoralis and Clavicular Clostridial Infection |
| 15754 bone clavicle sternum muscle pectoralis major sternoclavicular joint clavicular fx air fx swollen fx induration air bubbles dx clostridium welchii dx wet gangrene infection CTscan Davidoff MD 15754 15755 15758 15759 15759c01 |
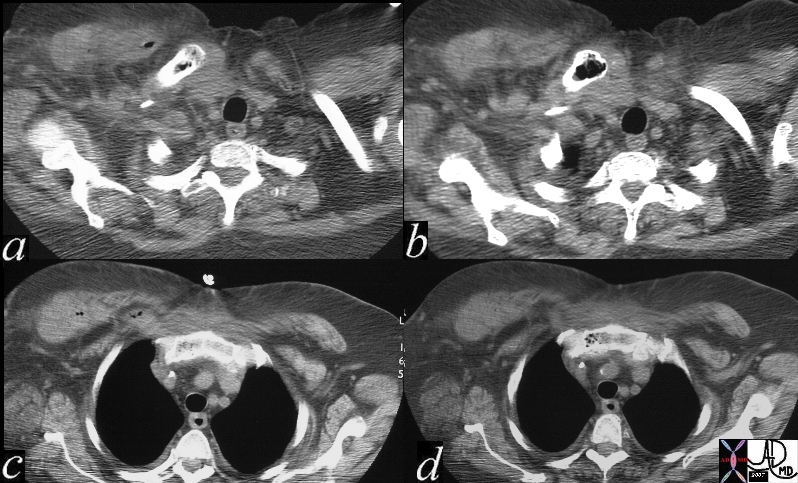
Clostridial Infection |
| 15759c01 bone clavicle sternum muscle pectoralis major sternoclavicular joint clavicular fx air fx swollen fx induration air bubbles dx clostridium welchii dx wet gangrene infection CTscan Davidoff MD 15754 15755 15758 15759 15759c01 |
References
Elstrom J, Virkus W, Pankovich (eds), Handbook of Fractures (3rd edition), McGraw Hill, New York, NY, 2006.
Koval K, Zuckerman J (eds), Handbook of Fractures (3rd edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Lieberman J (ed), AAOS Comprehensive Orthopaedic Review, American Academy of Orthopaedic Surgeons, 2008.
Moore K, Dalley A (eds), Clinically Oriented Anatomy (5th edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Wheeless’ Textbook of Orthopaedics: Clavicle Fractures (http://www.wheelessonline.com/ortho/clavicle_fractures)