
Assistant
Definition
By Gregory R. Waryasz, MD
The ulna of the musculoskeletal system is characterized by being the osseous stabilizer for the elbow joint. It is longer than the radius and more medial.
It is part of the upper limb. The ulna is part of the elbow and distal radial-ulna joint (DRUJ). It consists of bone and cartilage tissue once mature.
Its unique structural features include its being larger proximally than distally. The bone is relatively straight at the shaft. An interosseous membrane helps to connect the radius and ulna shafts. The ulnar shaft contains a narrow medullary canal.
The proximal ulna has two prominent projections; the olecranon and the coronoid process. The olecranon is located posteriorly and forms a prominence that can be felt just deep to the skin. The coronoid process is an anterior projection. The combination of the olecranon and the coronoid process helps to form the trochlear notch where the humerus articulates.
The tuberosity of the ulna is the site of attachment of the brachialis muscle.
The radial notch is the site of the articulation with the radial head. The supinator notch is inferior to the radial notch. The supinator fossa is a concavity where the supinator muscle attaches.
The shaft of the ulna is thick, cylindrical, and relatively straight. The diameter tapers as the ulna becomes more distal.
The distal ulna enlarges into the head of the ulna. On the head of the ulna is the small, conical ulnar styloid process.
The muscles that attach to the ulna are the triceps brachii, anconeus, brachialis, pronator teres, flexor carpi ulnaris, flexor digitorum superficialis, flexor digitorum profundus, pronator quadrates, extensor carpi ulnaris, supinator, abductor pollicis longus, extensor pollicis longus, extensor pollicis brevis, and the extensor indicis muscle.
The ulna has one primary and two secondary ossification centers. The body is the primary ossification center. It appears at 8 weeks of fetal gestation. The distal ulna appears at 5 years and fuses at 20 years of age. The olecranon appears at 10 years of age and fuses at 16 years of age.The ulna as well as all other bones, muscles, and ligaments of the body are derived of mesodermal origin in embryo.
The function of the ulna is to serve as the main osseous stabilizer of the elbow joint. The coronoid process helps to prevent posterior elbow dislocation. The ulna also serves as a site of attachment for muscles and ligaments. In combination with the radius, the forearm is able to pronate and supinate.
Common diseases of the ulna include arthritis, fracture, dislocation, tumor, osteomyelitis, and osteoporosis.
Arthritis can occur at either the elbow or distal radial-ulnar joint. Common arthritis types that can occur at these locations include osteoarthritis and rheumatoid arthritis.
Fracture of the ulna can occur with trauma.
Dislocation of the elbow can occur with trauma.
Osteomyelitis is an infection of the bone usually due to bacteria.
Osteoporosis is a condition of decreased bone mineral density.
Tumors can either be primary or from metastasis. A few primary tumors that can occur in bone include leukemia, lymphoma, neuroblastoma, osteoblastoma, osteosarcoma, osteoid osteoma, enchondroma, and Ewing’s Sarcoma.
Commonly used diagnostic procedures include clinical history, physical exam, x-ray, MRI, bone scan, and CT scan.
It is usually treated with internal or external surgical fixation or non-operative approaches for fractures. Dislocations are usually treated operatively. Tumors can be treated with surgery, chemotherapy, and radiation. Arthritis is treated initially with physical therapy, NSAIDs, and steroid injections. An elbow replacement can help improve pain from elbow joint arthritis. Osteomyelitis is treated both surgically and with antibiotics.
References
Elstrom J, Virkus W, Pankovich (eds), Handbook of Fractures (3rd edition), McGraw Hill, New York, NY, 2006.
Koval K, Zuckerman J (eds), Handbook of Fractures (3rd edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Lieberman J (ed), AAOS Comprehensive Orthopaedic Review, American Academy of Orthopaedic Surgeons, 2008.
Moore K, Dalley A (eds), Clinically Oriented Anatomy (5th edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Wheeless’ Textbook of Orthopaedics: Ulna/Ulnar Shaft Fracture (http://www.wheelessonline.com/ortho/ulna_ulnar_shaft_fracture)
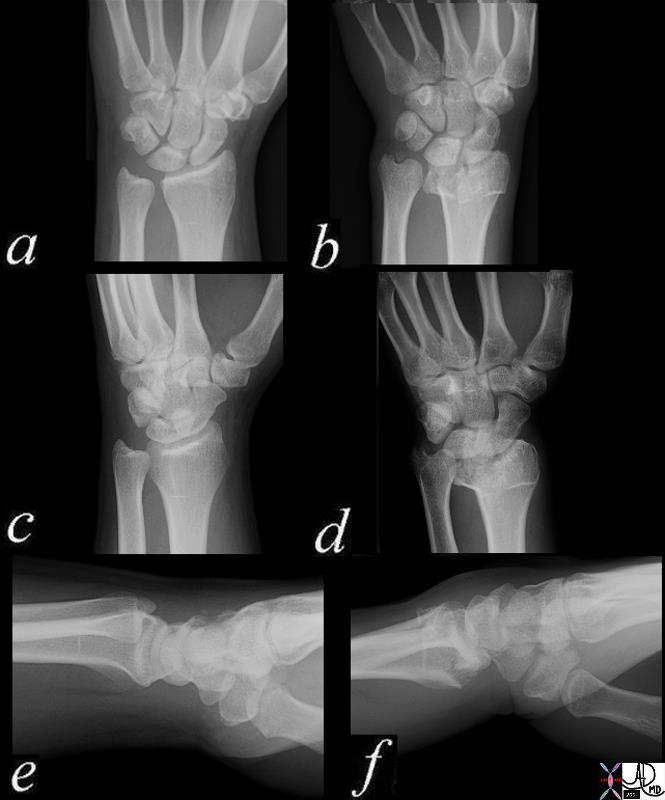
Normal and Colle’s Fracture |
| 70034c03 bone radius ulna wrist dorsally angulated fracture of distal radial metaphysis 2-3 cm proximal to wrist joint,sometimes associated frx of ulnar styloid frx line is almost always on volar side dx Colle’s fracture plain X-ray plain film of wrist normal wrist 70034c03 70034c04 Davidoff MD |

Mechanism for Colle’s Fracture |
| 85312p.800 falling outstetched arm Colle’s fracture mechanism of injury bone fracture Davidoff photography Davidoff MD |