
The Common Vein Copyright 2011
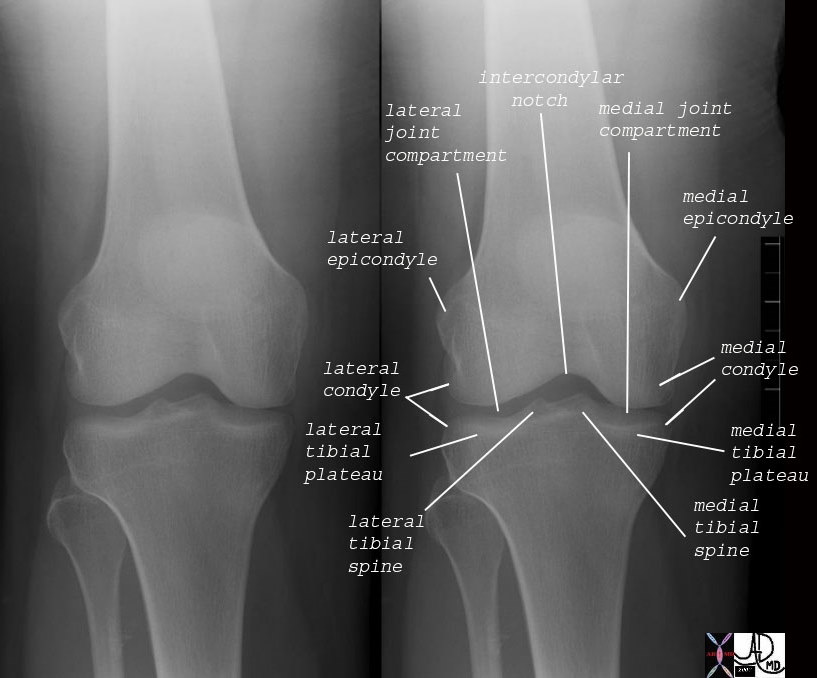
Bony Components of the Knee Joint – Small Parts
73478.c03 bone knee joint femur patella tibia fibula intercondylar notch lateral joint compartment medial joint compartment lateral epicondyle medial epicondyle lateral femoral condyle medial femoral condyle lateral tibial condyle medial tibial condyle lateral tibial plateau medial tibial plateau lateral tibial spine medial tibial spine normal anatomy plain X-ray Courtesy Ashley Davidoff MD 73478.c02 73478.c03
Definition
The knee joint is part of the musculoskeletal system and is characterized by being the largest and most superficial joint. It is a;lso charcaterised by its position and function of connecting the thigh to the lower leg.
It is part of the lower extremity and consists of bone, skeletal muscle, cartilage, synovial tissue, and tendon.
Structurally it is made from the the distal femur, proximal tibia and patella. There are three articulations; medial and lateral tibiofemoral and the patellofemoral articulation. The fibula is not involved in articulation. The joint is covered by a capsule. There is an internal synovial membrane that lines everything that is not covered with articular cartilage. The quadriceps femoris muscles provide the most stability to the knee joint.
The fibula is not involved in articulation but serves as a support for the joint. The fibular/lateral collateral ligament acts in this capacity.
The ligaments of the knee include the patellar ligament, fibular/lateral collateral ligament (LCL), tibial/medial collateral ligament (MCL), oblique popliteal ligament, arcuate popliteal ligament, anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), transverse ligament, posterior meniscofemoral ligament, and the coronary/meniscotibial ligaments.
The menisci are fibrocartilaginous discs that are located between the tibia and femur. There is a lateral and a medial meniscus.
The lateral support structure for the patella is known as the lateral patellar retinculum. The lateral retinaculum is made up of two layers; the superficial oblique retinaculum and the deep transverse retinaculum. The superficial oblique retinaculum receives fibers from the patellar tendon, vastus lateralus, and iliotibial band. The deep transverse retinaculum consists of the epicondylopatellar band/lateral patellofemoral ligament, the midportion, and the patellotibial band.
The medial support structure for the patella is known as the medial retinaculum. There are three ligaments present in the medial support structure; the medial patellofemoral ligament (MPFL), the medial patellomeniscal ligament (MPML), and the medial patellotibial ligament (MPTL). The MPFL along with the vastus medialis obliquus form the primary restrictive mechanism for lateral patella deviation.
There are at least 12 bursae around the knee. They bursae are the suprapatellar, popliteus, anserine (pes anserine), gastrocnemius, semimembranosus, subcutaneous prepatella, subcutaneous infrapatella, and the deep infrapatellar.
The blood supply is from the genicular anastomoses and venous drainage is from the accompanying veins. The genicular anatomoses arise from the femoral, popliteal, and anterior and posterior recurrent branches of the anterior tibial recurrent and circumflex fibular arteries.
The innervation is from the nerves supplying the muscles going across and that act at the joint according to Hilton’s Law.
The knee joint’s components as well as all other bones, muscles, and ligaments of the body are derived of mesodermal origin in the embryo.
The function of the knee joint is for flexion, extension, gliding, rolling, and rotation. When the knee is fully extended and weightbearing, the knee “locks”. Locking is due to medial rotation of the femoral condyles on the tibial plateau. The locking function is important to allow the muscles to relax during standing. Unlocking occurs when the popliteus contracts to rotate the femur laterally 5 degrees. This allows for flexion.
Knee extension is primarily from the quadriceps femoris and weakly by the tensor fascia lata.
Knee flexion is performed by the hamstrings (semimembranosus, semitendinosus, biceps femoris) and weakly gracilis, sartorius, gastrocnemius, and the popliteus.
Medial rotation is performed by the semitendinosus and semimembranosus when the knee is flexed primarily. When the non-weightbearing knee is extended the popliteus performs medial rotation. The gracilis and sartorius are secondary medial rotators.
Lateral rotation is performed by the biceps femoris when the knee is flexed.
Common diseases of the knee joint include arthritis, bursitis, tendinitis, fractures, stress fractures, meniscal tears, dislocation/subluxation, septic arthritis, osteomyelitis, Blount’s disease, patellofemoral pain syndrome, iliotibial band syndrome, Baker’s cyst, and osteoporosis.
Bursitis can occur at any of the bursae of the knee due to overuse/friction leading to inflammation of the bursa.
Fractures can occur with the femur, patella, fibula, or tibia.
The medial or lateral menisci can become torn acutely or due to chronic degenerative changes.
The ACL, PCL, LCL, or MCL can be torn or strained from trauma.
The quadriceps or patellar tendon can be torn or have tendinitis.
Blounts Disease is a growth disorder of the medial proximal tibial physis resulting in a varus deformity (bowlegged).
Hoffa’s disease is inflammation of the infrapatellar fat pad.
Plica synovialis is a condition of folds of embryonic synovial membrane remnants that can lead to pain if they do not degenerate as they are supposed to in the developing fetus.
Bipartite patella is a variant of the patella when there is a second ossification center. It occurs more commonly in men. It is often mistaken for a fracture.
Patella baja and alta refer to the anatomic relationship of the patella to the femur. Alta is a high riding patella and baja is a low riding patella. These can be symptomatic or asymptomatic.
Patella dislocation/subluxation typically occurs laterally due to the stronger lateral restraints. Often the medial patellofemoral ligament is injured.
Patellofemoral pain syndrome (PFPS) or runner’s knee is a common cause of anterior knee pain where there is abnormal tracking of the patella leading to increased contact pressures of the patella on the femur.
Chondromalacia patella is a softening and degeneration of the cartilage under the kneecap.
Sinding-Larsen-Johanssen disease is a condition of pain at the inferior pole of the patella in preteen boys due to traction on the patella by the patellar ligament.
Osgood Schlatter is a condition of juvenile traction osteochondritis where there is partial avulsion of the tibial tuberosity. It tends to be more common in early adolescent boys.
Transient synovitis or toxic synovitis is joint pain after a recent viral illness or trauma. It is a self-limiting condition of patients ages 3 to 8 years.
Lyme Arthritis is a condition common in the northeast USA where there is a rheumatologic reaction to Borrelia burgdoferi. It occurs after the patient is bitten by a tick.
Osteomyelitis is an infection of the bone typically caused by a bacteria.
Septic arthritis is an infection of the synovial tissue of the joint with pus in the joint cavity. The infection is capable of rapidly destroying the joint.
A Baker’s cyst or popliteal cyst is an accumulation of synovial/joint fluid behind the knee. It may cause pain and/or rupture.
Commonly used diagnostic procedures include clinical history, physical exam, x-ray, CT, and MRI. Ultrasound can be used to help with diagnosis of effusion and synovial thickening.
It is usually treated with rest, NSAIDs, physical therapy, and surgery. Septic arthritis is treated with surgical washout and antibiotics. Arthritis and fractures can be treated with surgery including total knee replacement. Osteoporosis is treated with bisphosphonates, calcitonin, calcium, and vitamin D. Transient synovitis is treated with NSAIDs. Meniscal tears and articular cartilage injury can be treated with physical therapy or arthroscopy. The ACL, PCL, MCL, or LCL tears and strains can be treated operatively or non-operatively. Blounts Disease when it does not correct itself typically is corrected with a surgery on the growth plate. Sinding-Larsen-Johanssen and Osgood Schlatter disease are treated non-operatively with quadriceps strengthening exercises and other physical therapy modalities. Lyme Arthritis requires treatment with antibiotics. Patellofemoral Pain Syndrome is treated with physical therapy and NSAIDs.
Definition
The knee is the articulation between the thigh and the (lower) leg. It is a hinge joint, the largest in the body, that enable us to perform one of the most basic functions of our existence: ambulation.
Structurally it is characterised by its position as described, and functionally it suports almost tye entire weight of the body.. It plays a major role in locomotion, lifting, and protection.
Anatomical components:
a) Bones
i) Femur
ii) Tibia
iii) Patela
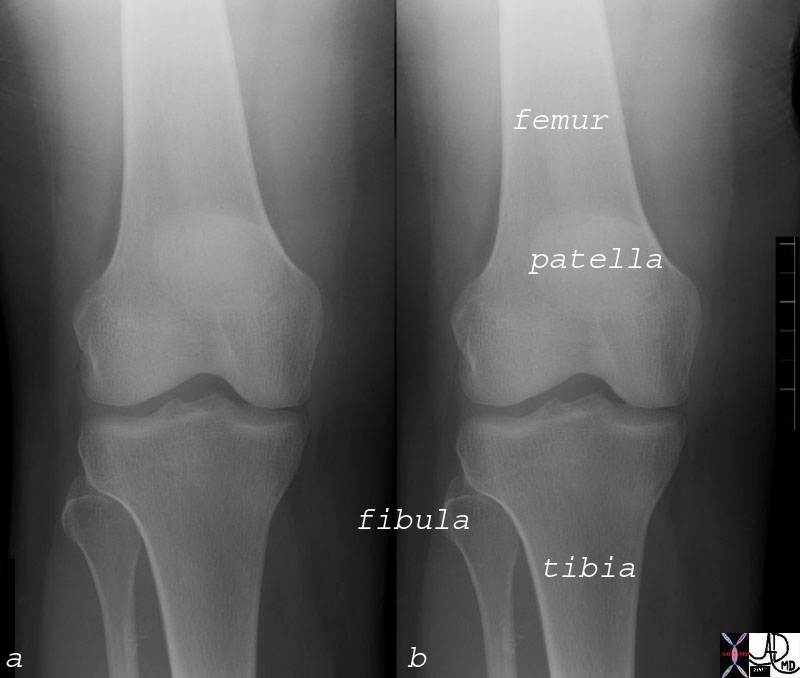
Bony Components of the Knee Joint – Big PArts |
| 73478.c02 bone knee joint femur patella tibia fibula intercondylar notch lateral joint compartment medial joint compartment lateral epicondyle medial epicondyle lateral femoral condyle medial femoral condyle lateral tibial condyle medial tibial condyle lateral tibial plateau medial tibial plateau lateral tibial spine medial tibial spine normal anatomy plain X-ray Courtesy Ashley Davidoff MD 73478.c02 73478.c03 |
b) Capsule / Bursae (12)
i) Subcutaneous prepatellar
ii) Subcutaneous infrapatellar
iii) Deep infrapatellar
iv) Suprapatellar
v) Gastocnemius
vi) Anserine
vii) Popliteus
viii) Semimembranous
c) Ligaments
i) Patellar
ii) Medial (tibial) collateral
iii) Lateral (fibular) collateral
iv) Coronary
v) Oblique popliteal
vi) Arcuate popliteal
vii) Anterior cruciate
viii) Posterior cruciate
d) Muscles
i) Quadracepts femoris
(1) Rectus femoris
(2) Vastis lateralis
(3) Vastis Medialis
(4) Vastus Intermedius
(5) Sartorius
(6) Gracilis
(7) Tensor fascia lata
ii) Flexors
(1) Semitendinosus
(2) Semimembranosus
(3) Bicepts femoris
(4) Gastrocnemious
(5) Plantaris
(6) Popliteus
e) Tendons
i) Quadracepts femoris
f) Cartilage / Meisci
i) Medial articular cartilage
ii) Lateral articular cartilage
iii) Medial meniscus
iv) Lateral meniscus
|
|
| Menisci of the knee joint. A. Superior view. Menisci of the knee joint. B. Normal knee joint showing the medial meniscus. T2-weighted magnetic resonance image in the sagittal plane. C. Normal knee joint showing the lateral meniscus. T2-weighted magnetic resonance image in the sagittal plane. |
g) Vessels
(1) Arteries
(2) Popliteal artery
(3) Descending branch, lateral femoral circumflex
(4) Descending geniculate
(5) Superior lateral geniculate
(6) Middle geniculate
(7) Superior medial geniculate
(8) Inferior geniculate
(9) Posterior tibal
(10) Anterior tibial
ii) Veins
iii) Lymphatics
h) Nerves
i) Femoral
ii) Tibial
iii) Common fibular
|
Bony Components of the Knee Joint – Small Parts |
| 73478.c03 bone knee joint femur patella tibia fibula intercondylar notch lateral joint compartment medial joint compartment lateral epicondyle medial epicondyle lateral femoral condyle medial femoral condyle lateral tibial condyle medial tibial condyle lateral tibial plateau medial tibial plateau lateral tibial spine medial tibial spine normal anatomy plain X-ray Courtesy Ashley Davidoff MD 73478.c02 73478.c03 |
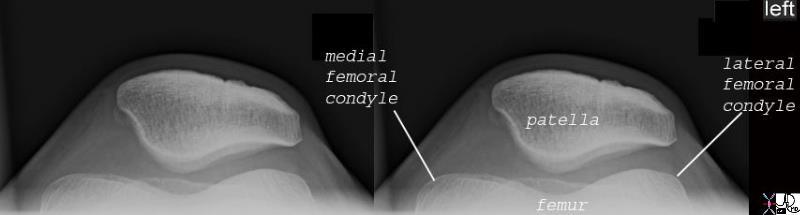
The Patella Sunrise View |
| 71223c02 71223.800 bone knee patella femur mdial femoral condyle lateral femoral condyle sunrise view plain X-ray normal anatomy Courtesy Ashley Davidoff MD |
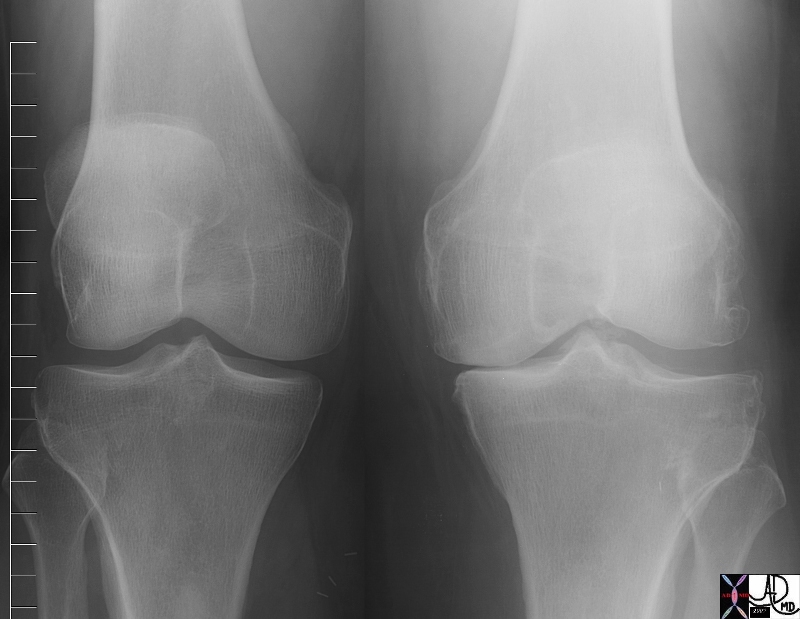
Normal and Degenerative Changes in the Medial Compartment |
| 71744b01.800 bone joint knee femur tibia tibial plateau normal joint space narrowing size degeneration of joint cartilage plain film X-ray Davidoff MD |
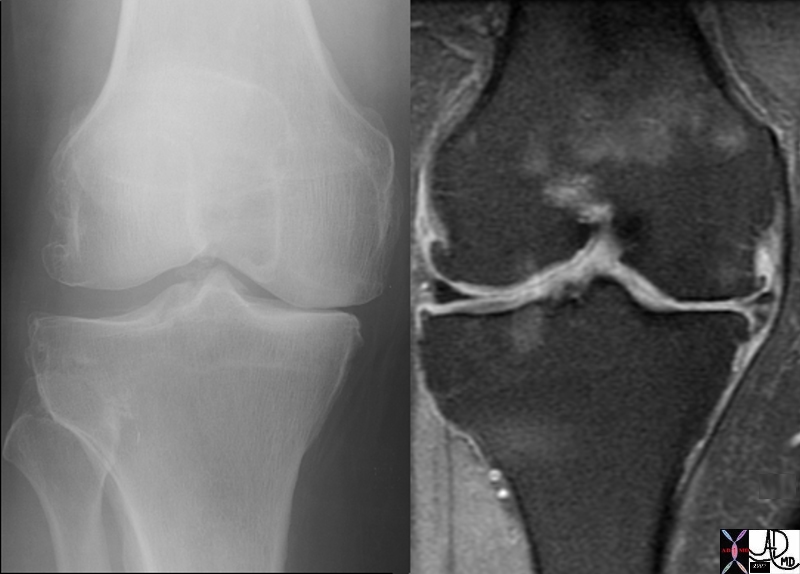
Degenerative Changes in the Medial Joint Space |
| 71744c01 bone joint knee femur tibia tibial plateau joint space narrowing size degeneration of joint cartilage plain film X-ray MRI T2 weighted image Davidoff MD |
References
Davis MF, Davis PF, Ross DS. Expert Guide to Sports Medicine. ACP Series, 2005.
Elstrom J, Virkus W, Pankovich (eds), Handbook of Fractures (3rd edition), McGraw Hill, New York, NY, 2006.
Koval K, Zuckerman J (eds), Handbook of Fractures (3rd edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Lieberman J (ed), AAOS Comprehensive Orthopaedic Review, American Academy of Orthopaedic Surgeons, 2008.
Moore K, Dalley A (eds), Clinically Oriented Anatomy (5th edition), Lippincott Williams & Wilkins, Philadelphia, PA, 2006.
Wheeless’ Textbook of Orthopaedics: Knee Joint Menu (http://www.wheelessonline.com/ortho/knee_joint_menu)
Links
Washington.edu Radiology Department